Over the last few days on facebook and across social media platforms, there has been the evocation of fear based in the findings from a new study around the evidence that high potency cannabis used daily may cause increase the risk for psychosis. While alarming at first glance, as someone who understands the endocannabinoid system and the benefits of cannabis, and as an advocate for patients’s rights to access this herbal medicine, I feel obligated to take a closer look at the evidence as presented in The Lancet. So feel free to join me on this journey of evaluating the evidence (or perhaps for those of you with advanced research analysis skills, take a look at the article yourself and see, regardless of your stance on cannabis, what the researchers did well and where they might be flawed). As President of the American Cannabis Nurses Association, my bias toward being pro-cannabis is clear, but I am also pro-patient and pro-safe use of cannabis, so I will do my best to provide an honest analysis. My approach here is the same that I would use in my work with my RN-BSN students, going through each area of the research, and using an approach to express my concerns that all levels of educated healthcare professionals can understand.
The full text article can be found here: https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(19)30048-3/fulltext
(Be sure to download the appendix as well, if you are following along!).
My thoughts are in blue font.
Title: The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe (EU-GEI): A multi center case-control study. (long title, but fairly clearly depicts what the study is about). The article is open access, which I like.
Journal: Lancet Psychiatry (reputable!)
Authors:Lots of good credentials here; a mix of MDs and PhDs. There are over 30 authors, which I find interesting. Sometimes this is a good thing, sometimes it doesn’t mean much. In the field of nursing, 30 authors would be quite large; in the world of physics hundreds to even thousands of authors can get credit…but are they really authors? Here is a link that looks at this issue (if you care or if your dare!), but this seems reasonable in this case: https://physicstoday.scitation.org/doi/10.1063/PT.3.1499
Funding: This was funded by the Medical Research Council, the European Community’s Seventh Framework Grant, Sao Paulo Research Foundation, the National Institute for Health Research Biomedical Research Center, Maudsley NHS Foundation Trust (South London and University College London), Kings College London, and Wellcome Trust.
At least five of the authors report funding from pharmaceutical companies, though stating that they were funded for other studies, not this study. Check out the full list at the end of the article. Getting funded is part of people’s jobs within research. Its just one of those little tidbits, to keep in mind, that certain loyalties and biases may be playing a part in the research here. “Big pharma” can be viewed as having vested interests in people using cannabinoids (which they may eventually be producing medicines for us all to use someday) or people sticking with their traditional allopathic medicines (I won’t get into the poly pharmacy issue and all of those implications) or even creating pharmaceuticals that help people managing psychosis.
Problem: In the beginning of the article, the authors state that with legalization movements, we may have “an increase in cannabis use and associated harm, even if the later only affects a minority of patients” (p. 1) and they go on to state that several studies “support a causal link between cannabis use and psychotic disorder”(p.1). Ideally I would have time to thoroughly analyze each of the 5 cited studies in the first paragraph, but seeing as nobody is paying me to do this work, I instead decided I would check out at least one of the articles cited. I went to the fifth article cited because of the researchers’ claim that the research may “support a causal link” (which was very concerning to me, because I keep running around saying “correlation is not causation…!” and people don’t seem to get that).
And it turns out that key word “support” is very important: when I reviewed the cited study by Gage, Hickman, and Zammit (2016) entitled “Association Between Cannabis and Psychosis: Epidemiological Evidence”, their conclusions lead me to believe that they did not determine causation. Gage at al basically looked at the evidence from longitudinal studies, and in their findings, they distinctly refrain from making a “causal” statement: “Overall, evidence from epidemiological studies provides strong enough evidence to warrant a public health message that cannabis use can increase the risk of psychotic disorders. However, further studies are required to determine the magnitude of this effect, to determine the effect of different strains of cannabis on risk, and to identify high-risk groups particularly susceptible to the effects of cannabis on psychosis”. When people read articles like this one we are analyzing here, it’s just too easy to assume that somehow causation has already been proved, when it clearly has not.
The authors in the introduction go on to state that there is a rising incidence of schizophrenia in the world. “Differences in the distribution of risk factors for psychosis, such as cannabis use, among the populations studied might contribute to these variations” (p. 1). Hmm, well, this might be related to cannabis use, but when I checked out the articles cited, they had more to do with income, urbanicity, migrant status, age, race/ ethnicity, and whether or not the person owned their home. I think we just have to be careful as readers and consumers of evidence to pay very close attention to the subtle nuances. What the researchers are saying is that they think cannabis should be examined in light if rising schizophrenia diagnoses (though some of the literature I read as part of this process stated that schizophrenia is not rising, rather its falling as we do a better job of differentiating and diagnosing). More on this later…
In a pink box on page 2, the authors summarize some of the previous work done in this area I found their review of the literature (I think that is part of the purpose of this box?), a bit compelling, though they only found 3 articles that matched their criteria for psychotic disorders in combination with specific terms like “high potency cannabis””skunk-super skunk” or “high THC cannabis”. Two of the articles were their own work, and the third article was much older, going back to 1965-1999 London where increasing rates of schizophrenia “might be related” to cannabis use in the previous year.
I couldn’t find the authors of this rise in schizophrenia article cited on the reference list, so I asked Dr Google for some help. I did eventually find the article and review the abstract…it then lead me to wonder about the idea of increasing diagnosis of schizophrenia during this time period, which then lead me to stumble upon a major issue with the criteria for schizophrenia, how it was historically diagnosed, and the argument that there may be some big issues around valid DSM criteria for the various types of schizophrenia (rabbit hole alert, check it out, check it out…https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5103459/). Though I worked in psychiatric nursing a few eons ago, I am clearly not up-to-date on all of the controversies that the DSM seems to spark.
As near as I can tell, “psychotic disorders” are pretty much undifferentiated, and this is why the authors used this term vs chasing a more definitive diagnosis like perhaps bipolar or schizophrenia, which may be more difficult to make and of course may take time to differentiate. According to the NIH/NIMH, “psychosis” describes conditions where the person has a mind condition, and they have lost contact with reality: it can be a sign of a mental illness or physical illness, it can be caused by medications/ alcohol/drug abuse, 3% of the population experiences it, and symptoms include hallucinations, delusions, paranoia, and disordered thoughts/speech. Studies show that is common for people to have symptoms for more than a year prior to diagnosis.
https://www.nimh.nih.gov/health/publications/raise-fact-sheet-first-episode-psychosis/index.shtml
This is extremely important to note because the researchers here looked at cases of first-psychosis, but there appears to be no follow-up regarding if these were “temporary” diagnoses, or if they persons were eventually diagnosed with schizophrenia or bipolar. They did use ICD-10 criteria to define the population eligible for the study : https://www.icd10data.com/ICD10CM/Codes/F01-F99/F20-F29/F20- but it remains vague to me as far as differentiating this population and they simply lumped all psychotic disorders together.
It is known that adverse effects of cannabis can be things like hallucinations and paranoia, so I started to worry a bit and wonder if these folks were high at the time of intake into the ER, and if they were experiencing adverse effects vs a mental health diagnoses. Thankfully, I do see some distinction of this in the article: if the symptoms were from acute intoxication, the person was not included in the study. Phew! I can assume they knew how to differentiate this.
Participants: Participants were people age 18-64, they were diagnosed using the ICD-10 criteria for psychosis (which envelops a lot, check out link above). Control groups were apparently randomly selected from the same area using postal address, age, race, gender, ethnicity, and lack of psychotic symptoms as the control criteria. The researches had participants in the 17 areas of England, France, the Netherlands, Italy, Spain, and Brazil. The researchers were striving to assess 1000 first time psychosis and 1000 controls. I did not see in the study that cannabis use was ever confirmed by a urinalysis or blood test. This seems obvious to me, but since they are looking a year back, maybe it’s not needed? I really would have liked to have known their current status of testing positive for cannabis.
The n for each group was good: control = 1237, cases= 901
Methods:
The researchers asked the participants about 6 measures of cannabis use: lifetime use (whether or not they ever used cannabis), current use, age at first use, lifetime frequency (pattern or most consistent use), money spent weekly (or during most consistent use period), The researchers then used data from the European Monitoring Centre for Drugs and Drug Addiction 2016 report to determine cannabis potency by THC. (download it, you’ll like it, it’s fascinating: http://www.emcdda.europa.eu/publications/edr/trends-developments/2016_en) , however, I actually ended up finding the data elsewhere on the website, where they have info about potency. The data available now is from 2018, I am assuming the researchers used 2016 data http://www.emcdda.europa.eu/data/stats2018/ppp_en.
Okay, wait, what, don’t tell me…they didn’t ask the patients what specific strain they were using, nor actually test the cannabis strains the patients used, they conjectured from the data? I think I would have felt more comfortable if they would have collected some kind of data from patients beyond frequency of use that demonstrated that they were actually, truly consuming high potency cannabis. Additionally, I had to dig around the website to find the potency, and the data is not well labelled.
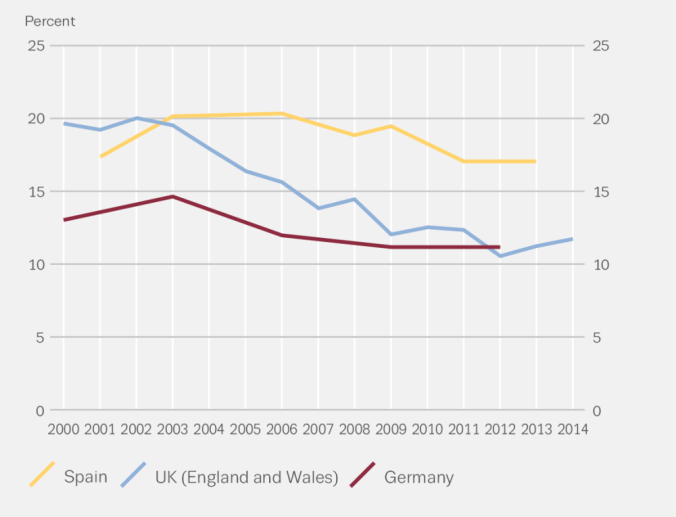
Also, another discovery in the EMCDDA report (figure 2.1) tends to show a downtrend in cannabis use in Europe, particularly in the 3 countries that previously were high prevalence countries such as Germany, Spain, and the UK. So while cannabis may be getting stronger, it’s use sure has dropped off greatly since the year 2000 in these 3 countries (which perhaps goes against the researchers thoughts that cannabis use is on the rise and posing a greater risk for psychosis).
EMCDDA (2016).
Back to the Methods. I am directed to the appendix to further investigate how they determined “high potency”. I am feeling frustrated, because there is no appendix on the pdf I downloaded, and luckily I did find it on the main page. The appendix has lots of great further details and I am left to wonder why the editors had them put this crucial data in the appendix.
Based on the data, low potency cannabis was <10% THC and high potency cannabis was >10% THC. Participants were asked to report the type of cannabis used, in their own language, and potency was estimated based on the data from EMCDDA. The participants seemed to give what I can only categorize as broad terms for the cannabis they were using, including UK home-grown skunk/sensimilla UK Super Skunk, Italian home-grown skunk/sensimilla , Italian Super Skunk, the Dutch Nederwiet, Nederhasj and geimporteerde hasj, the Spanish and French Hashish (from Morocco), Spanish home-grown sensimilla, French home-grown skunk/sensimilla/super-skunk, and Brazilian skunk. (To clarify, in the UK “skunk” is a term used for all high THC % cannabis plants, but I could not find a clear definition for “skunk” in terms of strains or exactly what the cut off is for a plant to be called skunk). https://www.independent.co.uk/news/uk/home-news/uk-cannabis-market-skunk-drug-strength-weed-spice-street-sales-dealers-a8231426.html
This process of asking data based questions of patients experiencing first time psychosis brings up red flags for me: firstly, asking patients who are in first time psychosis what “type” of cannabis the participants were using seems highly unreliable to me. The problems with patients and participants self-reporting data are well known, and yet this whole study is about self report, I get it…we may not have better ways to collect the data (yet), but it remains an issue for me. They did also have some other questions around intoxicants, which is good, but I will get back to that with results.
Secondly, the actual cannabis was never tested for true potency (back to the idea of the researchers claiming these patients used high potency cannabis, but the only evidence of them doing so was that they may have consumed cannabis in a geographical area where high potency cannabis is available), nor was there any indication that the patients were tested for THC (granted they could have tested negative and last use could have been some months before the episode).
What about the actual findings????
Hang on for Part II of the analysis! The findings and conclusion analysis coming up in Part II!
References:
European Monitoring Centre for Drugs and Drug Addiction. (2016). European Drug Report 2016: Trends and Development. Retrieved from http://www.emcdda.europa.eu/publications/edr/trends-developments/2016_en
Forti, M.D., Quattrone, D., Freeman, T.P., Tripoli, G., Gayer-Anderson, C., Quigley, H….et al. (2019). The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe (EU-GEI): a multicentre case-control study. The Lancet, Psychiatry. Open Access. DOI:https://doi.org/10.1016/S2215-0366(19)30048-3
