Our July gathering to focus on networking among Black, Indigenous, Latina/x and other nurses of Color is happening on July 31st! For this and all of our meetings going forward, register on Zoom to get the meeting login details. You can register right up to the time the meeting starts, and if you lose the meeting information – just register again!!
During August, our organizing team is taking time for an intensive retreat to plan for the future of this project. During this time, we will post on this blog every Thursday with information about the future of our work together, and will include resources that everyone can tune in to as we continue to grow in our capacity for anti-racism activism in nursing!
To begin, we are featuring “Anti-racism Daily” – a daily newsletter that gives important information about the many ways that you can raise your awareness and grow your activism! Take a look at the amazing list of archives – there are topics covered here that many of us have never even imagined in the context of our anti-racism awareness!
Throughout the history of professional nursing, nurses have designed new care delivery models and transformative interventions in response to unmet needs and population health and public health challenges. These changes required disruptive thinking and bold courage in the face of broken systems, ineffective policies, and powerful naysayers. Climate change may be a modern example of a major public health crisis yet the challenges to mounting an effective response are similar. This is the story of Nurses Drawdown, a global, nurse-led movement to improve the health of humans and the planet.
Honoring the Ancestors of this Movement
Around the globe, the earliest experts in planetary health were, and continue to be, indigenous people. Their values and patterns of decision-making acknowledge the deep interconnection of human health and the health of the biosphere.
Many early nursing leaders shared a similar awareness that we ignore the environment at our peril. The ideas of Florence Nightingale, Lillian Wald, and Mamie Odessa Hale offer inspiration to transformative leaders today. Florence Nightingale is considered the founder of modern professional nursing; her astute observations and applied statistics established nursing as a science-based profession. Nightingale was an expert systems thinker who connected the health of humans to the quality of the environment. Like Florence, nurses today must recognize that nursing care is delivered in the context of nature.
Lillian Wald
Lillian Wald, the founder of public health and school nursing, faced the daunting task of addressing the health needs of resource-poor immigrants in New York City (Wald, 1915). She went to the people and lived among them. Her willingness to participate in health initiatives alongside those she served offers a lesson for transformative leaders today. Nurses can inspire people to take action on climate change by first making changes in their own lives.
Mamie Odessa Hale was another historical change agent. Hale was an African American Nurse Midwife practicing in an era of deep racial segregation. She taught community midwives simple practices based on the best science of the time thereby improving birth outcomes for African Americans (Hale, 1948). The story of Mamie Odessa Hale encourages today’s nurses to realize that simple science-based interventions, taught with respect and empathy, can transform the health of individuals and whole communities.
These early nursing leaders laid the foundation for today’s global movement to address climate change. They are a part of the Nurses Drawdown story.
The Seeds of a Movement
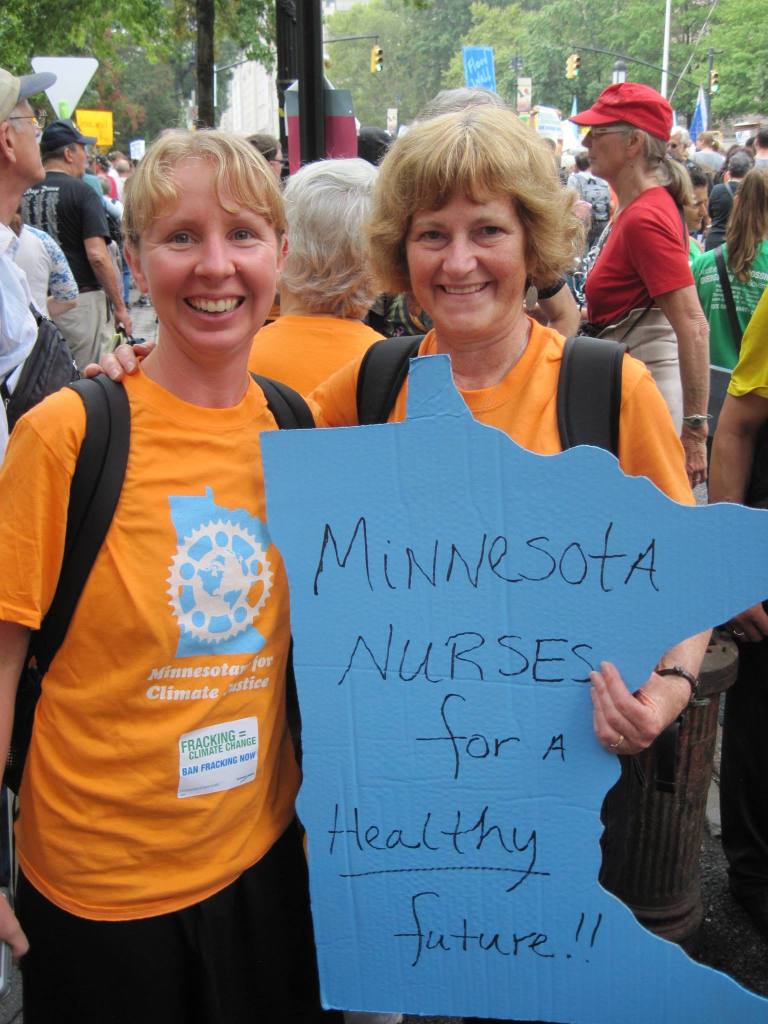
In September 2014, I took a long bus trip across the nation to attend the People’s Climate March in New York City. Over half a million people from all demographics and all walks of life came together to send a strong message that the United States must take climate change seriously and meaningfully contribute to global negotiations.
Like my fellow travelers from Minnesota, I wore a bright orange t-shirt. The only indication that I was a nurse was the sign I created that said, “Minnesota Nurses for a Healthy Future.” As the march moved through the streets of Manhattan, I was shocked how frequently observers standing along the route commented to one another, “The nurses are here!” Some even asked to take their picture with me so they could send it out on social media with the message that nurses had shown up to address climate change. I remember thinking, “What is this?” The people were not shouting, “The engineers are here!” or “The teachers are here!” There is something about nurses taking on climate change that inspired hope.
Fast forward to 2018 when I adopted the book Drawdown: The Most Comprehensive Plan Ever Proposed to Reverse Global Warning (Hawken, 2017) for “The Global Climate Challenge: Creating an Empowered Movement for Change,” a course that I teach at the University of Minnesota. Climate change is an urgent public health crisis; therefore, I teach that our solutions must be effective and have significant impact. Project Drawdown (2020)provides the solutions; could nurses provide the inspiration to scale them?
I contacted Project Drawdown and presented the argument that as the largest global health profession and the most trusted profession, nurses may be able to effectively and broadly scale Project Drawdown’s science-based solutions to climate change. Nursing’s long history of innovative leadership to improve the health of individuals, families, and communities can be relied on to improve the health of humans and the health of the planet. So, a partnership was formed between Project Drawdown and the Alliance of Nurses for Healthy Environments (ANHE).
ANHE (2019), the leading professional organization for nurses working to promote a healthier environment, coordinates the Nursing Collaborative on Climate Change and Health, a broad network of professional organizations committed to planetary health. Katie Huffling and Cara Cook from ANHE and I assembled a leadership team to plan and initiate Nurses Drawdown. It was very important that we include nurses across the globe, nurses from a wide variety of practice settings, and different demographics including nursing students.
Nurses Drawdown
The vision for Nurses Drawdown is “to improve the health of individuals, communities, and the planet through commitment to and action on the Nurses Drawdown solutions.” The mission is, “Nurses, the most numerous and most trusted health profession in the world, have the power to significantly impact climate change. By embracing and teaching the evidence-based solutions of Nurse’s Drawdown, nurses around the world will help to decrease greenhouse gas emissions and create a healthier future for humans and the rest of the planet.”
To this end, the Nurses Drawdown leadership team elected to scale Project Drawdown solutions that have the co-benefits of improving human health and the health of the planet. We selected five themes, reflecting an alignment between core nursing expertise and effective evidence-based solutions. These include:
FOOD: Committing to eat a more plant-based diet, using clean burning cookstoves, and reducing food waste
MOBILITY: Promoting walkable cities, including improving bike infrastructure and using mass transit
GENDER EQUITY: Educating girls and improving access to family planning
ENERGY: Increasing the efficiency of buildings and transitioning to clean energy sources
NATURE-BASED SOLUTIONS: Planting trees and protecting forests
An Invitation to Join the Movement
Throughout history, professional nurses have been at the forefront of change. Whether it was alleviating mass suffering related to conditions of war, addressing severe economic disparities that impact health, or responding to new and emerging infectious diseases, nurses’ orientation toward systems thinking and prevention have made them the ideal leaders for innovating and mobilizing effective solutions.
We invite you to continue this tradition by joining Nurses Drawdown at nursesdrawdown.org. Under the Take Action tab, you will find practical solutions to apply in both your personal and professional life. You will also be inspired by the stories of nurses around the globe who are taking action to promote a healthier future for generations to come.
Many will remember 2020 as the year of the pandemic. Let them also remember 2020 as both the Year of the Nurse and Midwife (World Health Organization, n.d.), and the year that nurses around the globe activated to address climate change. The nurses are here!
Clinical Professor, School of Nursing- University of Minnesota
Specialty coordinator of the Doctor of Nursing Practice in Health Innovation and Leadership
Director of Planetary Health
Dr. Potter is deeply committed to climate change education including co-founding Health Professionals for a Healthy Climate, membership in the Alliance of Nurses for Healthy Environments, and membership on the American Academy of Nursing Environment and Public Health Expert Panel. She is a member of the Coordinating Committee of Columbia University’s Global Consortium on Climate and Health Education and a Fellow in the Institute on the Environment at the University of Minnesota. She chairs Clinicians for Planetary Health (C4PH) and is a member of the Steering Committee of the Planetary Health Alliance at Harvard.
At the University of Minnesota, Dr. Potter designed and co-teaches an interdisciplinary course titled “The Global Climate Challenge: Creating an Empowered Movement for Change”. In addition, she co-leads a Health Sciences initiative titled, “Climate Change and Health: An Interprofessional Response”. In 2019, Dr. Potter was appointed the first Director of Planetary Health for the School of Nursing.
Social justice movements have historically incorporated arts based visual components to amplify their messages by using images and visual art to literally making the invisible more visible. Examples of this include Judy Chicago’s Dinner Party and the AIDS quilt.
As an arts based medium, quilts are powerful semiotic vehicles for protest and memory, and actual representations of comfort and care. Throughout history, suffragettes, abolitionists, enslaved people, Vietnam war protesters, and HIV/AIDS and 911 survivors have used fiber art and the quilt medium to come together in communal spaces for the purpose of grieving, memorializing and honoring others, and for communicating political opinions about important issues of the day.
This week, health care providers from the group called Doctors for Camp Closure, (D4CC) are coordinating a nationwide 24-hour protest vigils outside detention centers to draw attention to the serious risks of infection from CoVid-19 in detention centers and prisons nationwide. In solidarity and collaboration with community groups around the nation, D4CC are incorporating many arts based events including poetry reading, music, story telling, reflective journaling, and the creation of a virtual and actual protest quilt called the #D4CCQuiltProject.
Using the social media platform Instagram and the use of the project hashtags, the virtual #D4CCQuiltProject project will “sew” together images from the nationwide protest, banner messages, and other images or words drawing attention to the risks of CoVId-19 infection for detained and incarcerated people. The #D4CCQuiltProject can also spotlight less obvious historical and structural issues of the Capitalocene that are driving refugees to immigrate around the globe including persistent white settler colonialism, neoliberalism, militarization, persistent extraction of living and non living resources around the world by the Global North, and climate related extremes- all factors driving im/migration globally and to the US, and contributing to conditions of extreme poverty, violence, and food and water insecurity throughout the world. Structural violence issues
MIssion Statement: The #DetentionIsDeadly #FreeThemAll Quilt Project messages are intersectional social justice messages and may include these ideas among others :
Show healthcare worker support for the Free Them All movement to release people detained by ICE during COVID pandemic, draw media attention to the dangers of incarceration, and increase public support for decarceration
Prisons and detention centers are filled with impoverished Black and Indigenous People of Color, and Undocumented People, and they are increasingly the largest sites of COVID-19 infection
Social distancing in detention or prison to reduce the risk of COVID-19 is impossible.
As health care providers we oppose detention.
Many prisons and detention centers in the US are capitalist oppressive for-profit systems that filled with people who have been disadvantaged across generations by the very systems that now hold them prisoner.
Migration to the US is driven by intersectional issues for which we as US citizens are complicit including US colonialism, climate injustice, capitalist extractive industries, globalization and neoliberalism (think sugar, palm oil, hydroelectric power, coffee, lumber, beef, global agriculture to name a few).
Native American and Indigenous land rights issues in the US are erased within discussions of immigration. (One example among others is: May 2020 The Wampanoag Tribe in in Massachusetts are struggling to retain land rights).
LQBTQI issues get erased in the discussion of immigration and detention.
Project Vision
A virtual quilt that “sews” together square virtual images that align with the purpose of the action. and/or
An actual quilt that has names, images etc on fabric and that can be actually sewn together and/or
An intersectional art project that is open to the greater art community.
Project Guide: How to Participate
DIRECTIONS
There are TWO WAYS TO PARTICIPATE IN THE QUILT PROJECT
VIrtual Quilt
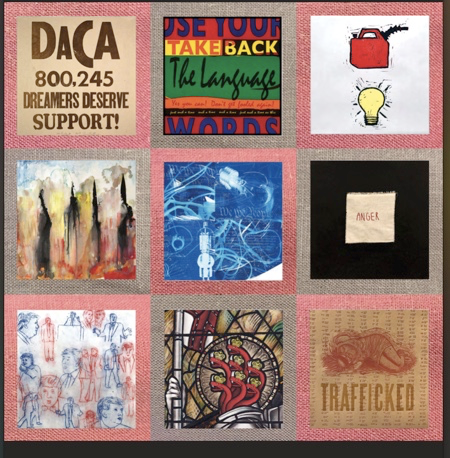
Take a square photo of any message or image that aligns with issues of social justice, examples above, open to interpretation; the only restriction is the photo/image must pass minimum standards for social media, ie) non vulgar non obscene etc
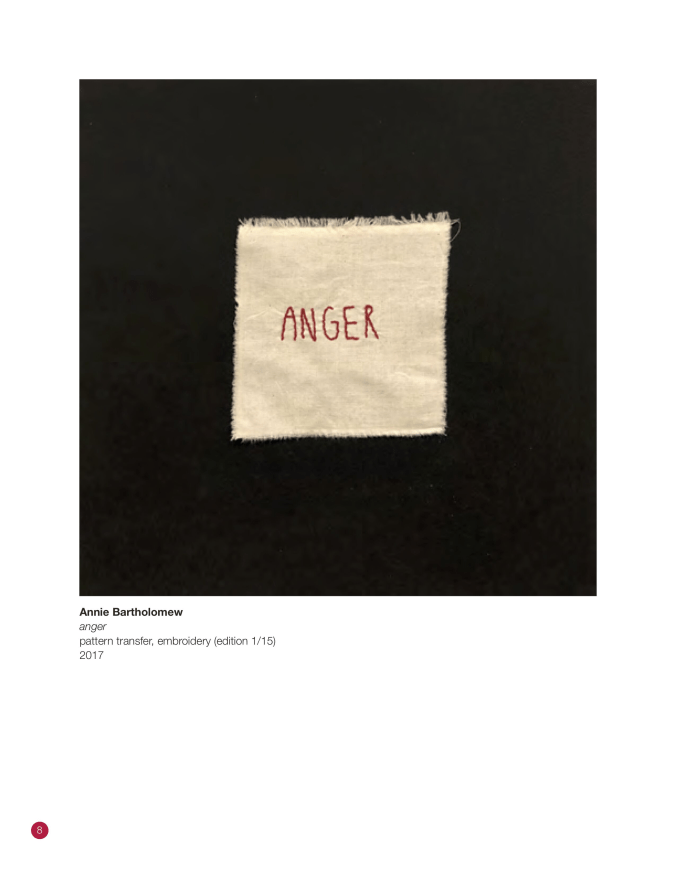
Can be poetry, single words or phrases, a photo of a flower, headline in news, anything, names of deceased persons to honor who have been impacted by structural violence, See some image examples below.
You may superimpose a message on a photo you already have. You may superimpose the project hashtags, or a message on a picture of your Protest Banner.
A Square image is needed to “fit them together “
Upload to Instagram with 3 primary hashtags #DetentionIsDeadly #FreeThemAll#D4CCQuiltProject
Secondary hashtags are fine too but you have to use these 3 so we can “find” the “images” on Instagram you can also Tag @doctorsforcampclosure
Ultimately, the images can be placed on colored squares see below and “sewn” virtually into a virtual quilt. This will happen in the near future after we have a number of images.
The quilt will be shared on social media to amplify the messages
Actual Quilt
During the vigil, before or up to two- four weeks after vigil, people can mail me 12 by 12 inch squares of actual fabric with messages hand written or sewn , and I will sew them together and make them onto a physical quilt.
Any fabric is acceptable but dimensions should be 12 inches by 12 inches
This is a way to get the public, friends, kids, and family members involved in this cause.
People can include the creation of a physical square as a way of reflecting during the 24 hour vigil. Think child art, spontaneous, no pressure to have any “art” or sewing skills. Just has to be about 12 by 12 fabric based no rules on type of fabric.
People can invite local community groups to participate in the creation of squares.
PM Jane Hopkins Walsh for address where to send fabric.
Fabric must reach me by +- June 15th 2020.
The actual quilt could be part of a larger traveling protest quilt that gets added on to in other future protests.
Ultimately the actual and the virtual quilt could be part of larger intersections with the art community to amplify and intersect our messages. For example we could have sew-ins in protest in NYC or other places, intersecting with other protests, or the quilt could travel to other cities and immigrant groups to include diverse social movements and groups all over. This is fluid and open to discussion as it unfolds.
EXAMPLES OF IMAGES BELOW- PLEASE IF YOU SHARE THESE IMAGES GIVE CREDIT AS LISTED BELOW.
Credit these 4 tags for this image above please @voxpopuliprintcollective @shimartnetwork #voxpopuliprintcollective #shimartnetwork
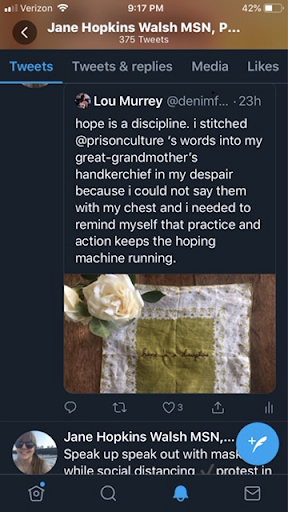
Credit for this image: from Twitter user@denimfemme Lou Murrey
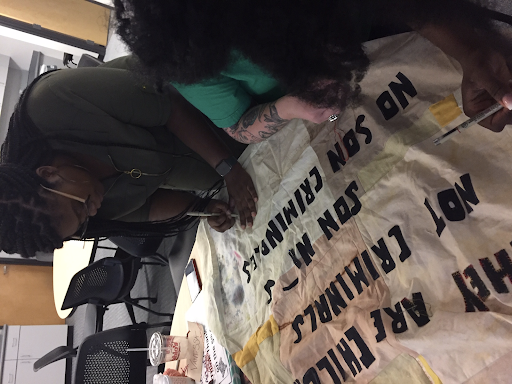
Credit for the quilt images are Instagram @janewalsh357 #BorderQuiltProject
Credit for the two quilt images above are Instagram @janewalsh357 #BorderQuiltProject
Credit for this image @voxpopuliprintcollective @shimartnetwork #voxpopuliprintcollective #shimartnetwork
About Jane Hopkins Walsh
Protest Opinions in this document are My own Pronouns She / Her Jane Hopkins Walsh MSN, PNPC Pediatric Nurse Practitioner Primary Care at Longwood Boston Children’s Hospital 300 Longwood Ave Boston, MA 02466 jane.hopkins-walsh@childrens.harvard.edu
Volunteer and Board Member Cape CARES Central American Relief Efforts www.capecares.org
PhD Candidate and Research Fellow Boston College William F. Connell School of Nursing Enrolled: Center for Human Rights and International Justice Lynch School of Education Jonas-Blaustein Scholar Cohort 2018-2020 walshjm@bc.edu
Ongoing Issues: By now, most of us know the obvious: nurses and other healthcare professionals do not have the PPE that they need to practice safely. Nurses are testing positive for COVID19. The Defense Production Act has not been activated to produce more PPE and ventilators, and nurses and other providers are even fired for speaking out about it or organizing ways to access more PPE (Doctors and Nurses Fired for Speaking Out ).
Nurses’ Skill Level: Nurses are worried about being asked to do work they aren’t prepared to do. A former student of mine, who has been in more of an administrative role, is extremely concerned with being asked to go back into a hands-on medical surgical or even ICU in a supportive role. Practicing beyond one’s skill level or expertise is just one area of concern that is likely to grow as more nurses become ill, or refuse to work, or are otherwise unable to work.
Volunteer calls: From California to NYC to Maine, nurses are being asked to submit their names to volunteer to work. Most of these nurses will be paid, and it is an effort to organize our resources.
Nurses on the Front Line: The stories I am hearing from nurses are war-time hell-like, maybe even worse then you have heard of if you don’t have direct contact with nurses on the front line.
An example is a story a friend of mine posted from his friend in NYC: in the ER, there may be 7-10 COVID+ vented patients waiting for ICU placement. Some patients are lying on the floor in the ER because there are no beds. People are being taken to rooms on the floors and passing away before they even get seen by a nurse on that floor. Medications like propofol, ketamine, versed, and fentanyl are being run without pumps because there are no more pumps. Supplies are running out. Med Surg nurses are being forced to run drips and vents that they have not been trained on.
Pay Issues: In Utah, nurses and doctors are being asked to take pay cuts, and there is concern that this will create a great deficit of providers in this state when professionals go elsewhere to work (Utah’s largest medical provider announces pay cuts). Meanwhile, note this lovely NYC serene skyline shot, with pay that must recognize the obvious inherent hazard pay for these positions.
(nurses recruitment add, contact information removed)
Populations and Outcomes:
Much preventative and maintenance care for those with chronic and even acute illnesses is now taking a back seat. A positive note is that telemedicine and telehealth are being used much more widely, and this may have a favorable effect on how we care for populations in the future.
Dr. Chinn forwarded a first-hand account to me of a nurse who is working in Brooklyn. She is concerned about how this illness is impacting Latinx populations, as they are often members of “essential worker” populations, and they also live in large households. This nurse states that these patients are at higher risk for death, and often experience death with less dignity. She also sees all staff getting sick, from direct care providers to janitors, and patient care technicians.
Anecdotally, in one social media group, I heard the nurses estimating that survival rate once a patient is ventilated is only around 14-20%. This is devastating to be surrounded around so much futile care and facilitating so much end of life care without perhaps the time and space it requires to do this well. (Edited: national statistics show a recovery rate of about 50% post ventilator initiation).
Heartbreak: I am hearing heartbreaking stories of nurses sending off their children to grandparents or ex-spouses, so they won’t be exposed in the household should the nurse become sick themselves or accidentally contaminate the household. Nurses who can’t hug or hold their loved ones are aching inside every day. Nurses dying. Nurses looking around at their colleagues and they might wonder, who will be the next to not be at work, which one of us might end up in the ICU? Nurses may know that much of the care they are providing is futile or palliative, which creates moral distress. I am very concerned when I hear of nurses working multiple shifts, with one nurse posting that she had worked 13 shifts in a row, another posting about minimal sleep, and losing 10 pounds already. They don’t have time to eat and when they go shopping, the stores are lacking in supplies. There is no question in my mind that nurses are being put at greater risk not only due to exposure, but also due to physical, mental, emotional, and spiritual stressors.
Post-Traumatic Stress: We could say nurses are stressed, or maybe we should just be truthful and say that nurses are being traumatized. I have great fears of nurses leaving the profession after this, and I also have great fears about the health of the population in general. I am fearful for those on the front lines without access to proper PPE. This sort of chaos we are experiencing may lead to positive change eventually, but for now, it’s extremely uncomfortable, painful, confusing, infuriating, and even disorienting.
We need to take good care of ourselves and take good care of one another.
I am reaching out with loving-kindness to all nurses:
There is so much going on that it’s really hard to summarize all of the issues. I welcome dialog and discussion of your concerns and what you are seeing and hearing about.
Nurses’ Shifting Thinking About Duty To Provide Services
I am seeing a shift in thinking with more nurses being willing to leave their jobs as they are not adequately protected: working without adequate PPE creates harm to self, others, and community. An emergency room doctor was fired for speaking out about his hospital’s response (US NEWS report). So these actions are not without their cost.
We are also seeing more and more healthcare workers testing positive for COVID19. What stands out to me is the over 160 healthcare workers in Boston have tested positive for COVID19 in these early days. (Boston Hospital Workers test positive) and 12 nurses in Chicago have tested positive for COVID19 Chicago nurses test positive for COVID19.
Nurses who are staying in the direct care workforce are often very frightened: they are staying because if they quit, they won’t’ get unemployment, they are fearful that they won’t find another job because they left their current job abruptly, they are the sole or majority breadwinners in their families, and they are afraid of losing their healthcare benefits. Some nurses may still feel the deep roots of historically being linked to self-sacrificing, or with links to nursing’s history of religious or military duty (I do anecdotally feel like I am seeing less of this as the pandemic crisis grows).
New Grad Nurses as a Resource: Dr. Chinn pointed out to me that one area that is not getting enough attention is the idea of new grad nurses being allowed to or recruited into practice early, perhaps even before sitting for NCLEX or even finishing their final exams. An example: A CNO in a large New Jersey medical facility is begging a Nursing Program Director to send her senior nursing students to the clinical site, the NLN is okay with this, but how can she, in good conscience, allow her students to be there without proper PPE? Her students who work as techs at this facility also convey the dire conditions in the facility. Also, her faculty, like most nursing faculty, is older (in this case, age 59 on average) with underlying health conditions, which creates a greater risk for them as well.
My ethical perspective answer to this is that unless adequate supervision and proper PPE can be assured, the students should not be allowed into theses settings, as they will ensure harm to self and others, and we must abide by our ethical responsibility to practice beneficence and nonmaleficence. In my own setting as a director of an RN-BSN nursing program, we decided to remove all of our students from all clinical settings, even though we had students who wanted to stay in these community settings, the risks do not outweigh the benefits.
I also think of the challenges of being a new grad nurse: there is so much to learn and process and in a crisis situation will this even be possible? Will we ultimately end up losing a large number of these new grad nurses to post-traumatic stress and illness? This seems to me to really be lacking an ethic of care toward a very vulnerable population, our new grad nurses.
Is Nursing Political?
I was reminded this week that nursing is of course political. I found an interesting posting about how very political Florence Nightingale was. Cynthia Sim Walter (March 22, 2020, facebook) stated that during the Crimean War, Florence was first known as the Lady with a Hammer; she fought for her nurses to have what they needed to provide proper care, and she beat down military storerooms with a hammer. I loved this quote: “Military leaders loathed her and feared her. She drank brandy with the soldiers, did statistics for fun, and had no respect for the politics of men,” (I did not fact check this).
Florence took physical action when nobody else would and her actions were a political act of rebellion to save lives in dire times.
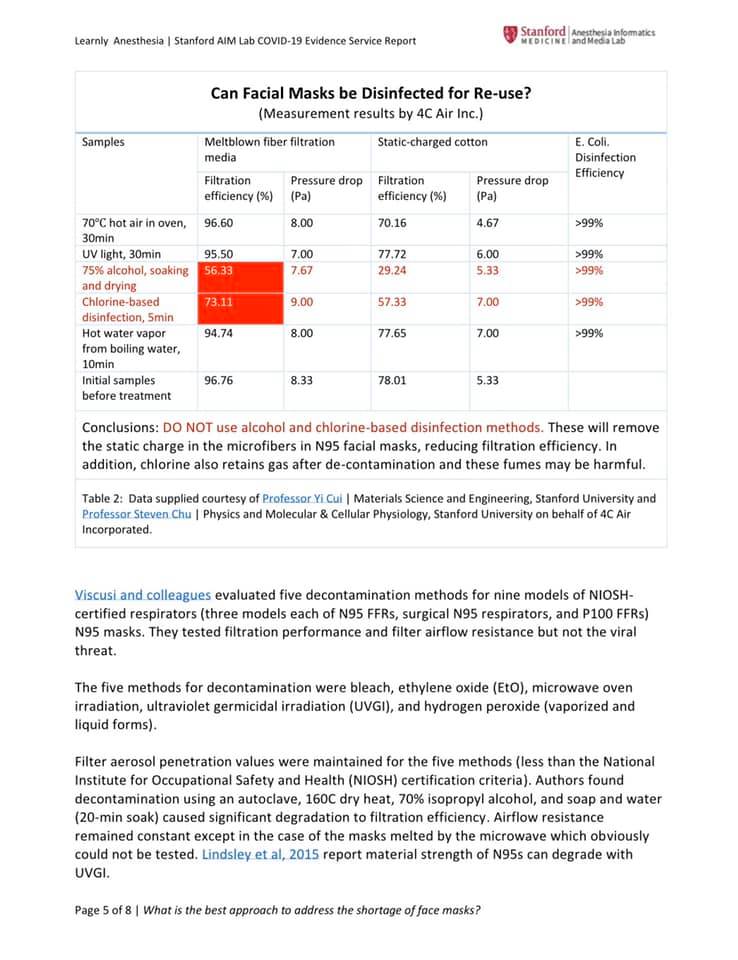
Let’s Reuse Our Masks? Here’s some data
This is heartbreaking when our leading facilities are looking for ways to somehow sterilize single-use masks. Here is something floating around on social media, put out by Stanford.
The full report can be read here. It sums up two important things, that autoclave may be effective (the mask will not have the same integrity, particularly over time; please see stats above). Also with the plastic face shields over other masks, we have no efficacy data around their effectiveness (Stanford Report).
We still need PPE to be well stocked so we can be more assured that we are well protected. We still need to be demanding that.
New Resources and Webinars:
To share more current information, the American Journal of Nursing has joined with Johns Hopkins and others to share ideas around keeping nurses safe. Here’s the link with all the info. https://nurses.wikiwisdomforum.com/
The Schwartz Center for Compassionate Healthcare is offering a webinar on Tuesday, April 7, 1-2 pm EDT, entitled: Leading with Compassion: Supporting Healthcare Workers in Crisis. Register Schwartz Compassion Center Webinar





 About Jane Hopkins Walsh
About Jane Hopkins Walsh